Clinical Case Series Summary
A frontline series in which the AAJT-S delivered non-invasive external aortic compression to combat casualties in traumatic cardiac arrest — achieving 100% ROSC.
Location: Ukraine
Clinical lead: Dr. Dmytro Androshchuk, Senior Lieutenant Ukrainian Armed Forces
Setting: Military & Tactical
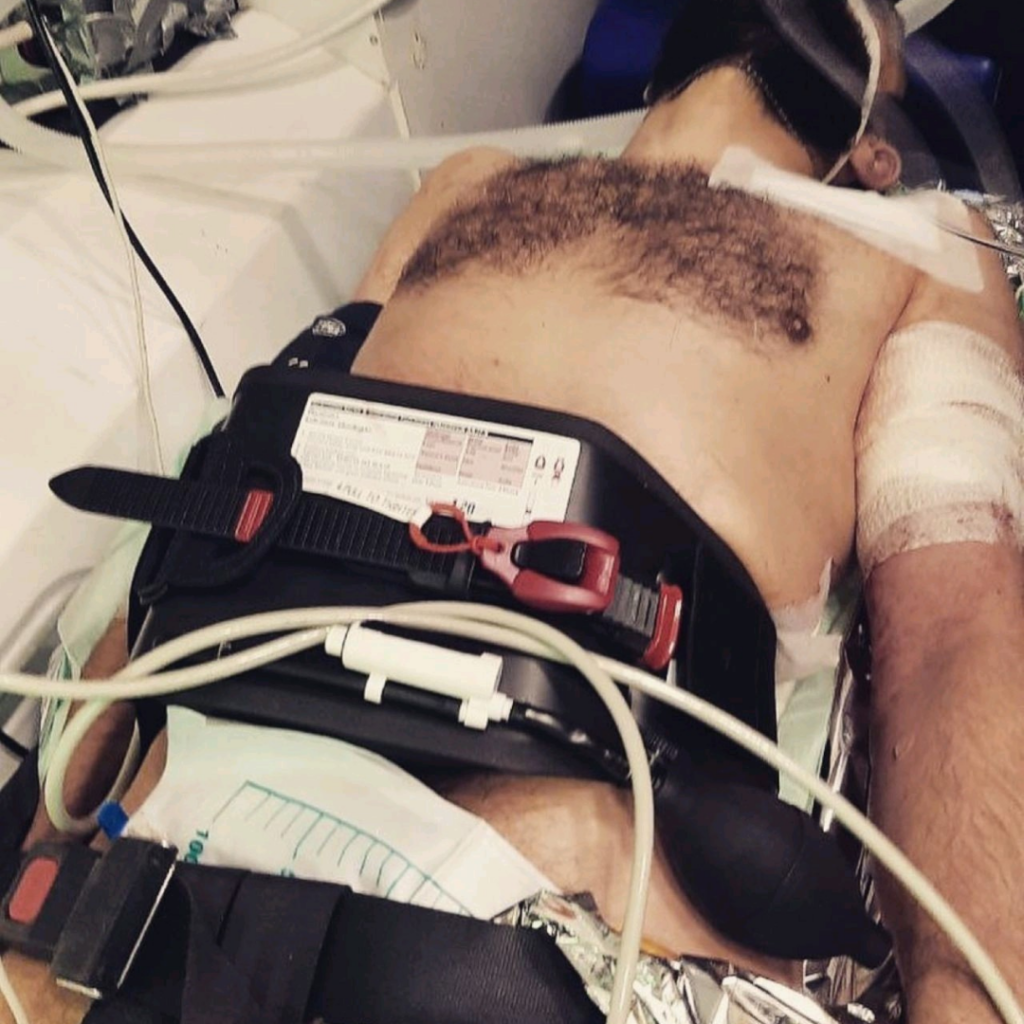
Application site: Abdomen (aortic compression)
Synopsis
- Severe hypovolemic shock
- Traumatic cardiac arrest (TCA)
- Austere combat environment
- AAJT-S at the umbilicus
- External aortic compression
- Increased mean arterial pressure
- Focused resuscitative efforts on the upper torso
- Preserved crucial field resources
- 100% ROSC (Return of Spontaneous Circulation)
- Hemorrhage controlled
- None required vasopressor support post-resuscitation
- Effectively managed TCA in a wartime FSSS
- MAP Increased
“The device simplified care and preserved resources, crucial in the field environment.“
— Dr. Dmytro Androshchuk, Senior Lieutenant Ukrainian Armed Forces, Vascular Surgeon, Senior Officer of Frontline Surgical Group
Prolonged warfare, limited medical resources, and extended evacuation times during the Russo-Ukrainian War have forced major adaptations in battlefield trauma care. Traumatic cardiac arrest (TCA) caused by exsanguination remains one of the leading potentially survivable causes of combat death, making rapid hemorrhage control and effective resuscitation essential when surgical intervention is delayed or unavailable.
This published case series describes six combat casualties treated at a Forward Surgical Stabilization Site (FSSS) following fighting near Bakhmut in 2022 and Slovyansk in 2023. Each patient presented in profound hypovolemic shock and subsequently developed traumatic cardiac arrest secondary to massive hemorrhage.
As part of their resuscitation, the AAJT-S was applied to the abdomen in all six patients to provide non-invasive external aortic compression and immediately control ongoing hemorrhage. Cardiopulmonary resuscitation (CPR) was initiated concurrently, along with transfusion of blood products in five patients and Lactated Ringer’s solution in one patient. Following resuscitation and removal of the AAJT-S, none of the patients required vasopressor support to maintain adequate blood pressure.
Hemorrhage control was achieved in every case, and all six patients experienced return of spontaneous circulation (ROSC). Five survived to the next level of care. Although two patients ultimately died from the severity of their injuries — one while awaiting evacuation and one after 10 days — four survived to hospital discharge. Long-term follow-up demonstrated that three survivors were neurologically intact at 18 months, while no death records matched the fourth patient’s identity and date of birth, suggesting long-term survival.
Clinical Impact: This case series highlights the potential role of external aortic compression as part of damage control resuscitation for traumatic cardiac arrest caused by exsanguination. By immediately controlling hemorrhage, increasing central perfusion, and concentrating resuscitative efforts on the heart and brain, the AAJT-S provided clinicians with valuable time to administer blood products and definitive care in an austere combat environment.
While larger studies are needed, these findings challenge traditional perceptions of survivability following traumatic cardiac arrest. The AAJT-S increased mean arterial pressure, focused resuscitative efforts on the upper torso, simplified care, and preserved crucial field resources. This series demonstrates that rapid hemorrhage control, combined with aggressive resuscitation, can result in meaningful survival — including neurologically intact outcomes — even under the extreme conditions of prolonged field care and delayed evacuation.
Published in the Journal of Special Operations Medicine (2025)
Successful Management of Battlefield Traumatic Cardiac Arrest Using the Abdominal Aortic and Junctional Tourniquet – Stabilized (AAJT-S)
Dmytro Androshchuk, Andriy Verba. J Spec Oper Med. 2025 Apr 4;25(1):65–69. doi: 10.55460/7FEV-3ZRK
Link to Full Case Report: https://pubmed.ncbi.nlm.nih.gov/40063952/